
Athletic Injuries 101: Golfers Elbow
 In this edition of Athletic Injuries 101, Dr. Sarah Ytsma explains the signs, symptoms, and treatment of golfers elbow.
In this edition of Athletic Injuries 101, Dr. Sarah Ytsma explains the signs, symptoms, and treatment of golfers elbow.
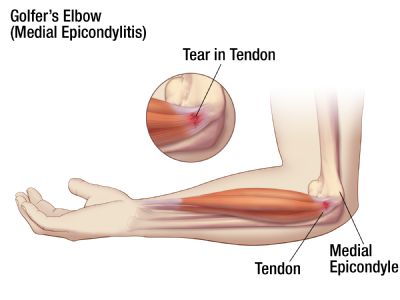
Golfers elbow is medically known as medial epicondylitis. It involves elbow pain on the medial or inside portion of the elbow due to inflammation of a tendon or inflammation of the muscle-bone-tendon attachment to the humerus. The most common site of pathology is the interface between the pronator teres muscle and the flexor carpi radialis muscle origins.
HISTORY/SIGNS/SYMPTOMS:
A) Golfers elbow is often associated with one of the following activities:
- Overhand throwing, tennis serving, golf swing, use of a hammer
- Sometimes begins with an acute strain but rarely from a single pitch, throw or swing.
B) It is often a gradual onset of pain, causing pain over the medial elbow
- Early –> pain with activity, relieved by rest
- Later constant pain with increased signs and symptoms with activity
- Eventually limiting/altering activity (can lead to shoulder and back problems too)
- Chronic pain may also accompany complaints of grip weakness
C) Morning pain and stiffness
D) Usually no visible swelling or deformity (other than hypertrophy or excess tension and size of muscle)
E) Tenderness on palpation:
- Young population –> pain is greatest over the medial epicondyle
- Adult population –> pain is greatest 1/2 – 1 inch distal to the medial epicondyle
F) Decreased range of motion and pain on active/passive elbow extension & supination at end range. Pain is usually worse with the wrist extended
G) Active ROM & resisted ROM – increased pain, decreased muscle strength of the following:
- wrist flexion – resisted
- Pronation – resisted
- Decreased grip strength – with pain\
H) Nerve function is not normally affected but this can be the cause of ulnar nerve problems
MANAGEMENT:
1) Acute – RICE protocol (Rest, Ice, Compress, Elevation) until pain subsides. Avoid aggravating and repetitive activities. Tape can be used to compress the elbow and/or wrist.
- Osseous manipulation/mobilization of the wrist, elbow, shoulder and neck as needed
- Muscle release on forearm
- Electrotherapy: ultrasound, IFC, TENS
- Acupuncture
2) Post Acute:
- begin throwing/activites when pain free
- strengthening activities with therabands/tubing/ TRX RIP Stick
- gradual distance throwing
- stretching of forearm, wrist, bicep
- taping the elbow or a compressive sleeve
- continued joint manipulation/mobilization, massage, electrotherapy as needed